Background
Hysterectomy/Myomectomy
A hysterectomy is the surgical removal of the uterus and is the most common of all gynecological procedures. A myomectomy is the surgical removal of uterine fibroids, or leiomyomas, and uses the same surgical techniques as a hysterectomy. Hysterectomy procedures can be sorted into three broad categories: abdominal hysterectomy (AH), vaginal hysterectomy (VH) and laparoscopic hysterectomy (LH). Laparoscopic and vaginal hysterectomies are preferred to laparotomies for several reasons:
Laparoscopic Hysterectomy
Traditionally, laparotomies were the only option for a hysterectomy, in which a large incision is made in the abdomen to remove the uterus. Recently, laparoscopic approaches to surgery have become more and more popular in the medical field. Not only do laparoscopic hysterectomies result in fewer complications (as mentioned above) but they also allow a clear view of the abdominal cavity, thus making this technique appealing to both the surgeons and patients.
Enlarged Uterus/Leiomyomas
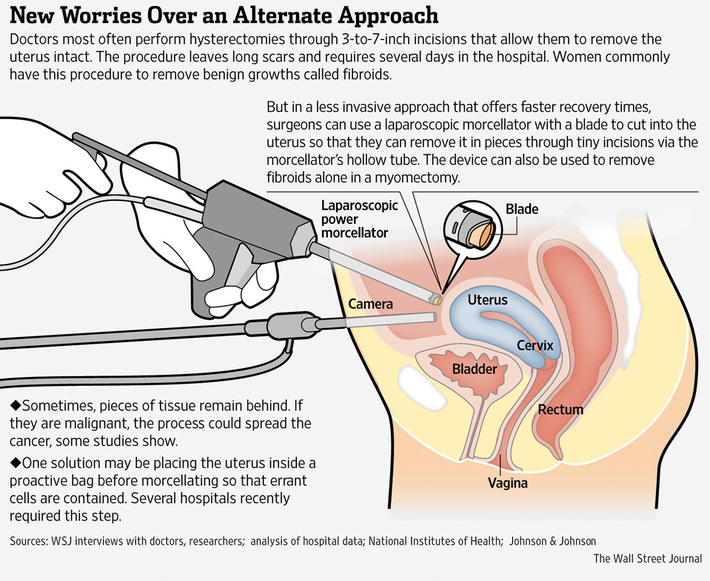
Sometimes, the uterus or leiomyoma will be too large to extract through an incision in the vagina, and therefore laparoscopic techniques must be used. The uterus or leiomyoma must be divided into smaller pieces, and one way to do this is using a power morcellation system.
Power Morcellation Systems
In laparoscopic hysterectomies/myomectomies, in order to remove the specimen it must be made small enough to extract through small trocars. The power morcellation system grips the tissue while a rotating blade fragments the tissue [1]. During this process pieces of tissue may be disseminated throughout the peritoneal cavity [2]. Therefore, if an undiagnosed occult malignancy was morcellated, it could spread to other parts of the body and potentially affect a patient’s prognosis.
A hysterectomy is the surgical removal of the uterus and is the most common of all gynecological procedures. A myomectomy is the surgical removal of uterine fibroids, or leiomyomas, and uses the same surgical techniques as a hysterectomy. Hysterectomy procedures can be sorted into three broad categories: abdominal hysterectomy (AH), vaginal hysterectomy (VH) and laparoscopic hysterectomy (LH). Laparoscopic and vaginal hysterectomies are preferred to laparotomies for several reasons:
- Decreased recovery time
- Less blood loss
- Quicker return to full activities
- Lower risk of surgical infection
- Less postoperative pain
- No large abdominal incision
Laparoscopic Hysterectomy
Traditionally, laparotomies were the only option for a hysterectomy, in which a large incision is made in the abdomen to remove the uterus. Recently, laparoscopic approaches to surgery have become more and more popular in the medical field. Not only do laparoscopic hysterectomies result in fewer complications (as mentioned above) but they also allow a clear view of the abdominal cavity, thus making this technique appealing to both the surgeons and patients.
Enlarged Uterus/Leiomyomas
Sometimes, the uterus or leiomyoma will be too large to extract through an incision in the vagina, and therefore laparoscopic techniques must be used. The uterus or leiomyoma must be divided into smaller pieces, and one way to do this is using a power morcellation system.
Power Morcellation Systems
In laparoscopic hysterectomies/myomectomies, in order to remove the specimen it must be made small enough to extract through small trocars. The power morcellation system grips the tissue while a rotating blade fragments the tissue [1]. During this process pieces of tissue may be disseminated throughout the peritoneal cavity [2]. Therefore, if an undiagnosed occult malignancy was morcellated, it could spread to other parts of the body and potentially affect a patient’s prognosis.
Source: [3] Levits, Jenifer, and John Kamp. "How Morcellators Simplified the Hysterectomy but Posed a Hidden Cancer Risk." 11 April 2014 2014.Web. <http://online.wsj.com/news/articles/SB10001424052702304432604579473362527708066>.
Needs
As mentioned above, power morcellation can spread undiagnosed cancer, as the tissue specimen is being fragmented uncontained in the abdomen [2]. Therefore, the ability to contain the specimen prior to morcellation is a large safety issue. However, using laparoscopic techniques to contain a sizeable specimen is not easily accomplished, especially in a timely manner. Therefore, a containment device should be constructed that is easily insertable and removable through minimally invasive incisions, and will not tear or rip when coming in contact with the morcellation device.
Project Scope
The goal of this project is to design a containment system that decreases the duration of laparoscopic hysterectomy/myomectomy for power morcellation procedures by at least two minutes. This system must be capable of entering and exiting the abdominal cavity through a 15mm trocar. Also, the bag associated with this system must be durable and resistant to puncture from the laparoscopic instruments.
Justification
Uncontained morcellation in laparoscopic surgery has been linked to increased cancer risk in patients. However contained morcellation still has a high rate of failure. Furthermore, contained morcellation increases operative time, which increases the cost of surgery. As uncontained morcellation is under scrutiny by the FDA because of increased cancer risk, the most advantageous improvements should occur in bag deployment efficiency.
Technical Requirements
To assist surgeons in performing laparoscopic hysterectomies/myomectomies we will design a containment system that meets these technical requirements:
- Bag must be flexible
- Should not cause any extra internal bleeding
- Costs $60- $100 per minute in the OR
- Maximum bag price = (current cost of bag) + $60 for every minute saved using the containment bag in the operating room.
- The system must be non-toxic, biocompatible, and sterile.
- System deployment must not injure the patient during insertion or removal through trocars.
- Bag must be flexible
- Should not cause any extra internal bleeding
- The bag must be waterproof and durable enough to withstand poking and prodding of standard laparoscopic surgical tools.
- The number, size or placement of incisions currently used in contained laparoscopic morcellation procedures will not be increased.
- The device will be capable of insertion through a 15mm abdominal trocar, and capable of extraction through the umbilical port. Therefore the device must be less than 15mm in diameter.
- The bag will be 50cm on each side, so that a range of specimen sizes will fit inside.
- The bag will be positioned using standard laparoscopic tools so that the opening of the bag faces upwards, towards the umbilical port, once it is inside the abdominal cavity
- The bag must be capable of being opened using standard laparoscopic tools when inside the abdominal cavity.
- Insufflation of the bag will take place through the pre-existing insufflation port on either the umbilical or side trocar.
- Closing the bag will be done through the use of standard laparoscopic tools.
- As the bag will be discarded after every use, it should be priced competitively to existing bags:
- Costs $60- $100 per minute in the OR
- Maximum bag price = (current cost of bag) + $60 for every minute saved using the containment bag in the operating room.
